Hello All,
As I wrote in Part One, nearly everyday, new members join our PPN Support,
Education and Advocacy Group. Their most important concerns are about getting
treatment to stop or manage their symptoms/paralysis and/or getting a
diagnosis. I have already written articles about how to find a good doctor and
how to get a diagnosis, which may take many years, but to this point have not
written about how to identify and eliminate the triggers that set off our
symptoms and paralysis.
As I have written before, there is no magic drug or cure
for Periodic Paralysis. There is an off-label drug that only works for a few
mutations and even then, there are and can be, serious side effects, long term
side effects and most individuals continue to experience paralysis and
symptoms. So despite having a diagnosis and possibly taking the off-label drug,
most individuals need to know how to manage their symptoms and episodes of
paralysis, because most triggers continue to set these things into motion.
For those still waiting for a diagnosis and hoping for
drugs/treatment from a “specialist” the diagnosis will probably not bring a
successful treatment. So, while waiting for a diagnosis, or if one has a
diagnosis and is on the off-label drug and still experiencing symptoms or if
someone has a diagnosis but cannot tolerate the off-label drug; the best way to
manage the symptoms and paralytic episodes to is identify the causes or
triggers for those symptoms and episodes.
This is part two of a Blog Article about how to identify and eliminate triggers.
From our book: The Periodic Paralysis Guide and Workbook:
Identify And Eliminate Triggers
AVOID - CHART -
JOURNAL - MONITOR
- Record symptoms and possible causes
- Monitor symptoms
- Keep a journal
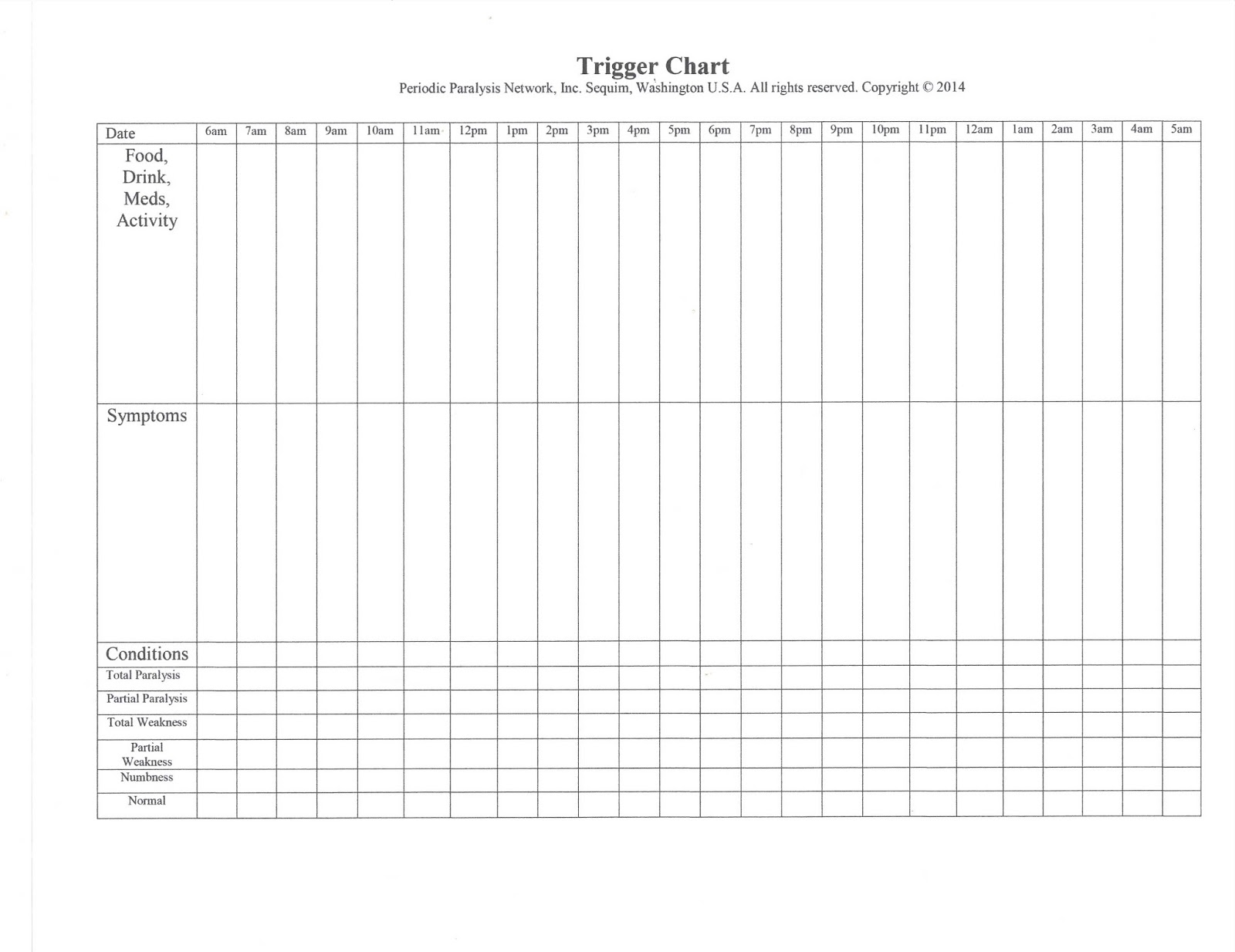
Fill in the date.
- Begin recording your activities, food, drink and medications in the top section. Start at the time you wake up. Include all food eaten in a meal. Record what you are doing, for instance sitting, eating, reading, exercising, walking, cooking, shopping or more.
- Record how you are feeling, for instance, good, very thirsty, constipated, confusion, sleepy, unsteady, legs are weak, total paralysis or more.
- Put a check mark in, (or fill in) the box that best describes your condition, for instance normal, weak, more weak, partial paralysis, more partial paralysis, or total paralysis.
- Continue this through your day, it is not necessary to do it at night, but you may want to include paralysis, numbness, or more, if it is happening at night.
- The bottom of the chart will become a graph and it will aid in seeing the times of symptoms.
In the completed chart below, we
can see that two and one half to three hours after eating breakfast and taking
septra, an antibiotic and a calcium tablet, the patient begins to experience
weakness and then paralysis. It is a good chance
that the medication or something eaten at breakfast was the cause.
If this person eats the same
thing everyday and takes the calcium every morning, and the only new thing is
the septra it would be safe to assume the antibiotic caused the episode. By
four pm the episode has stopped. At five pm muscle weakness begins after an
hour of being up and preparing dinner. This may be from exercise intolerance or
due to something eaten at lunch.
If someone eats the same lunch
everyday but does not always help with dinner, it could be safe to assume the
exercise caused the weakness. The same could be true in reverse. At seven pm,
overall weakness takes hold for the remainder of the evening. This may be from
the food eaten at dinner or a continuation of the weakness from the earlier
activity. During the night there are three episodes of total paralysis. Since
sleep is a trigger, it may be impossible to stop the episodes throughout the
night.

Evaluating the Data
When looking at your completed charts, it is best to first
check the periods of paralysis. Then check the activity, medications taken or
food eaten two to three hours before that time. Was anything new? Was any activity
out of the ordinary?
- Check period of paralysis or weakness:
- Check two to three hours before.
- New medication?
- New food, drink?
- New activity?
- More than usual?
- Longer than usual?
- If answer is not clear: Continue to chart for a few days. If there seems to be a pattern:
- Change only one thing at that time:
- Remove sugar or
- Cut medication dose or
- Stop or reduce the activity
- Less than usual
- Shorter than usual
- Check again after a day or two. If the symptoms of paralysis are reduced or better, you may have found the trigger. If not, add the thing you removed or reduced back into the meal, etc. Then repeat and change something else:
- Change only one thing at that time:
- Remove sugar or
- Cut medication dose or
- Stop or reduce the activity
- Less than usual
- Shorter than usual
- Repeat until you find the trigger or triggers.
Some suggestions for how to avoid the triggers once they are
found:
- On feet too long? : Break the activity in several shorter periods on feet.
- Cannot eat sugar? : Stop and try sweeteners, honey, stevia, etc.
- Cannot eat certain food? : Find replacement or do without.
- Cannot take medication? : Cut dosage, stop taking or get a replacement (under supervision of medical professional).
- Sitting too long? : Get up every hour or less and move around.
- Sitting too long? : Exercise in chair.
- Dehydrated? : Drink more water, set timer.
- Hungry? : Eat several smaller meals.
- Too hot? : Wear looser, cooler clothes, use neck cooler.
- Too cold? : Add clothing layers, use a blanket, drink hot drinks.
- Cannot drink caffeine: Drink decaffeinated drinks.
As the triggers are discovered and eliminated the attacks
of paralysis and other associated symptoms will begin to decline. The quality
of life will improve. The information will be recorded and can be shared with
the doctors and used as a tool during the diagnosing process. Use the following
blank page to record your own triggers as you discover them.
Monitoring the Triggers and Symptoms
Once many of the triggers have been established and a
diagnosis has been obtained (or not), it will be necessary to continue to
observe and monitor the symptoms and the triggers. As we have discovered from
my our experience and that of others with Periodic Paralysis, the triggers may
change over time or what may have seemed to be the cause, may not actually be
the cause. It is important to keep track continually in order to regulate and
control the symptoms.
For instance, at first it may appear that sugar eaten in a cookie is the culprit causing attacks of muscle weakness or paralysis. Later it may be discovered that it was actually the white flour or the chocolate in a cookie that may have caused the episode. Accidentally, it may be figured out that a person might be able to eat small amounts of sugar in a gluten-free cookie. Then after eating the gluten free cookie everyday for three days, a paralytic episode occurs. This may be that too much was eaten. So, it may be that small amounts of sugar may be eaten occasionally, just not everyday.
It is a fine line that an individual with Periodic
Paralysis must walk everyday. We must move through life as if we are walking a
tightrope. It has been said that when we figure out what our triggers are, we
must treat them as if they are allergies, something we must avoid. However, it
becomes a problem when those things are important elements needed in the body
such as salt or sugar.
In discussion with other individuals, we also have
discovered that surprising things may actually cause an attack. We may believe
we are doing everything correctly and avoiding all triggers and then we
suddenly slip into full body paralysis. This happened to me recently. I tripped
on my oxygen cord and landed on my knees. I scraped up one of them, but
otherwise felt fine. Three hours later I was in full body paralysis.
After discussing this with a friend and wondering what had
caused this attack, he reminded me that adrenaline is released when the body is
stressed or experiences some trauma. I realized that although I did not notice
much when I fell except a small scrape to my knee, my body had recognized it as
trauma, released adrenaline and three hours later I was paralyzed and for the
following several days.
Now I will remember that if I fall again, no matter how small or uneventful it may seem, I must prepare for the possibility of slipping into paralysis. I will be sure to rest and hope it will neither happen again nor be as serious as the last time. Better yet, I need to be more careful, now that I know if I fall, I will go into paralysis (or break a bone knowing I have severe osteoporosis).
Monitoring or keeping track of
triggers is important because it seems as if they are always changing and maybe
they are or maybe it is the amount of something we are using, but also it may
be that we have misinterpreted one trigger for another. We must use the charts
to keep track of symptoms and possible triggers and put them together in a
journal. The information in the charts and journal will be recorded and can be
shared with the doctors and used as a tool during the diagnosing process or for
treatment options.
Until later...


{kind=link}